
![]()

Robert W Malone MD, MS
This important preprint needs to hit alternative and mainstream media now.
The Study:Background: Previously, we demonstrated that ivermectin use as prophylaxis for COVID-19 was associated with reductions in COVID-19 infection, hospitalization, and mortality rates, and in the risk of dying from COVID-19, irrespective of regularity and accumulated use of ivermectin, in an observational, prospectively obtained data from a strictly controlled city-wide program in a city in Southern Brazil (Itajaí, SC, Brazil) of of medically-based, optional use of ivermectin as prophylaxis for COVID-19.
In this study, our objective was to explore the data obtained from the program to evaluate whether the level of regularity of ivermectin use impacted in the reductions in these outcomes, aiming to determine if ivermectin showed a progressive dose-, regularity-response in terms of protection from COVID-19 and COVID-19 related outcomes.
Materials and methods: This is a prospective observational study of the program mention above, that used ivermectin at a dose of 0.2mg/kg/day for two consecutive days, every 15 days. We obtained and analyzed the data regarding the accumulated dose of ivermectin use, in addition to age and co-morbidities, to analyze the patterns of reduction of COVID-19 infection, hospitalization, and mortality rates, and risk of dying from COVID-19, according to the regularity and amount of ivermectin used in a 5-month period.
Following definitions of regularity, we considered as strictly regular subjects that used at least 180mg of ivermectin (180mg = 30 tablets), and as sporadic users subjects that used 60mg (= 10 tablets) or less during the 5-month period.
Comparisons between subjects that did not use ivermectin and these two levels of regularity of ivermectin use were performed. Analysis of the intermediate levels of ivermectin use are present in the supplement appendix of this study. To analyze hospitalization and mortality rates, we utilized the database of COVID-19 infections of all participants, from Itajaí and outside. To analyze COVID-19 infection rate and risk of dying from COVID-19 we utilized the Itajaí city database.
Propensity score matching (PSM) was employed, followed by multivariate adjusted analysis for residual differences (doubly adjusted analysis).
Results:
- Of the 7,345 cases of COVID-19, 3,034 occurred in non-users, 1,627 in sporadic users, and 289 in strict users, while the remaining cases occurred in the intermediate levels of ivermectin use. Strict users were older (p < 0.0001) and non-significant higher prevalence of type 2 diabetes and hypertension.
- COVID-19 infection rate was 39% lower among strict users [4.03% infection rate; ( p < 0.0001] than in non-users (6.64% infection rate), and non-significant 11% reduction compared to sporadic users (4.54% infection rate) (n = 1,627 in each group; RR, 0.89; 95%CI 0.76 – 1.03; p = 0.11).
- Hospitalization rate was reduced by 100% in strict users, compared to non-users and to sporadic users, both before and after Propensity score matching ( p < 0.0001).
- After Propensity score matching, hospitalization rate was 35% lower among sporadic users than non-users (RR, 0.65; 95%CI, 0.44 – 0.70; p = 0.03).
- In propensity score matched groups, multivariate-adjusted mortality rate was 90% lower in strict users compared to non-users (p = 0.003) and 79% lower than in sporadic users (p = 0.05), while sporadic users had a 37% reduction in mortality rate compared to non-users (p = 0.043).
- Risk of dying from COVID-19 was 86% lower among strict users than non-users (p = 0.006) and marginally significant, 72% lower than sporadic users (p = 0.083), while sporadic users had a 51% reduction compared to non-users (p = 0.001).
Conclusion: Non-use of ivermectin was associated with a 10-times increase in mortality risk and 7-times increased risk of dying from COVID-19, compared to strictly regular use of ivermectin in a prospectively collected, strictly controlled population.
A progressive dose-response pattern was observed between level of ivermectin use and level of protection from COVID-19 related outcomes and consistent across different levels of ivermectin use.
The results of this study clearly demonstrate that prophylactic use of ivermectin must be initiated immediately for people in high risk categories in the United States and worldwide. This includes individuals with one or more co-morbidities and the middle aged/elderly. Our “design-to-fail” government funded clinical trials for early treatment and governmental obstructionism regarding life saving treatments to patients must end now.
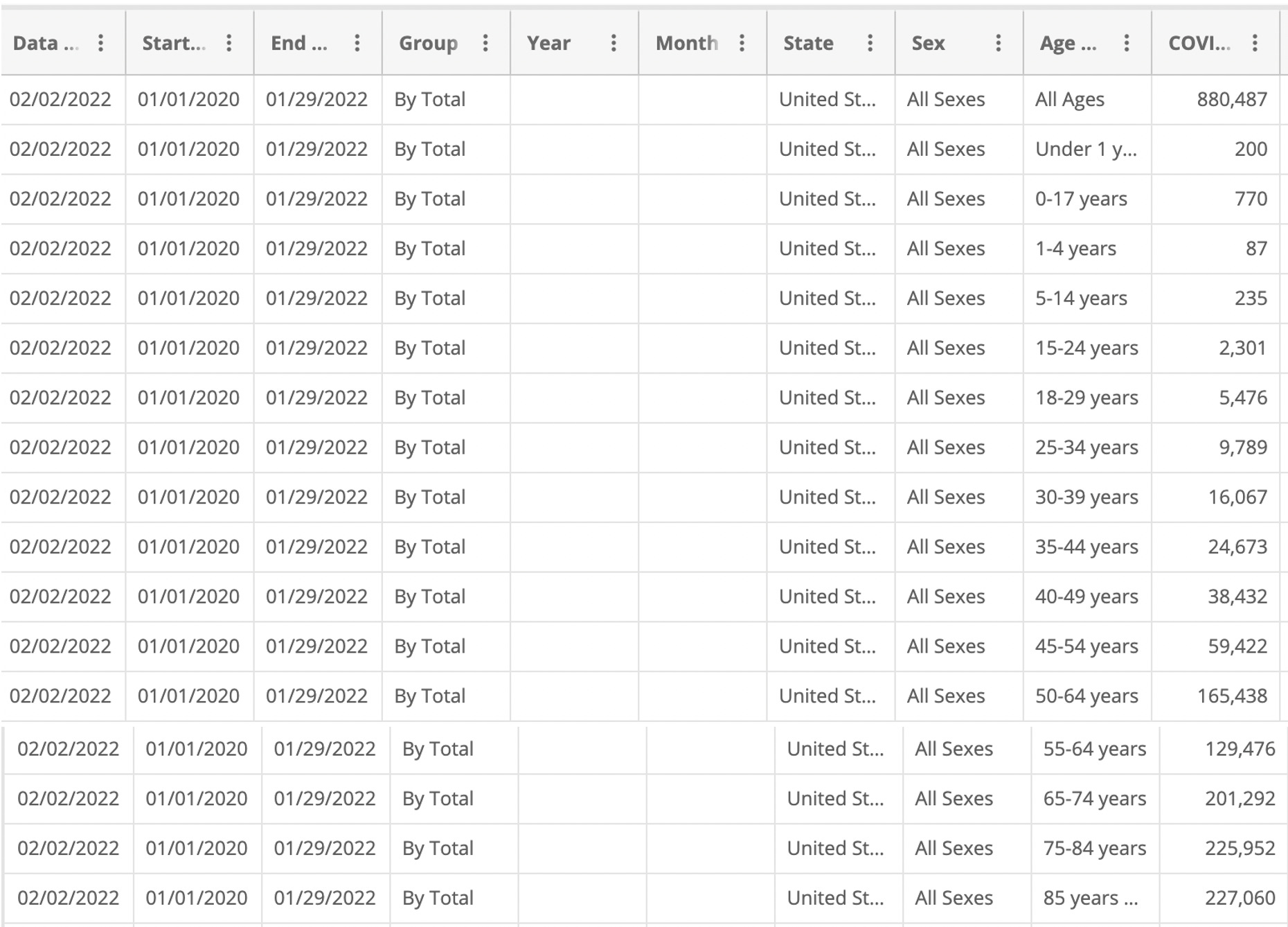
The CDC chart below for all deaths since the start of the outbreak clearly shows a jump in deaths after 50 years old.
However, as the data for deaths per million per age group is not disclosed, so the age for start of prophylaxis has yet to be determined.
As Omicron has less pathogenicity and slightly different disease profile this too could influence what age prophylaxis treatment should begin. But the data are in, prophylactic use of ivermectin saves lives.
In regards to the table above, the age stratification of disease shows why a universal vaccination program for a vaccine with a high adverse event profile is not advised. It is time to stop all mandates at the Federal and State level. It is time to stop pushing this vaccine on children.
Research and clinical practice show that using re-purposed drugs for Covid-19 have huge benefits. These include multi-drug, multi-staged treatments for Covid-19 disease that prevent severe disease, decreases hospitalization rates and decreases death. It is time our government and state licensing board recognize this and let physicians practice medicine.
‘Off-label’ drug use: an FDA regulatory term, not a negative implication of its medical use. Int J Impot Res. 2008 Mar-Apr;20(2):135-44. doi: 10.1038/sj.ijir.3901619. Epub 2007 Nov 15. PMID: 18004389.
Highlights:
- A doctor’s decision to inform the patient of the ‘off-label’ status of the prescription is not relevant to the physician’s standard of care for an informed consent case.
- The FDA has specifically stated that its procedures and requirements have no effect on the practice of medicine and that the FDA does not prohibit doctors from prescribing drugs in an ‘off-label’ manner.
- The FDA’s approval of a drug is immaterial to the effectiveness in the drug’s ‘off-label’ use. In fact, prescribing medication in an ‘off-label’ manner can constitute the standard of care in many cases.
- A doctor’s duty is to practice medicine and treat his patient, not inform the patient of the FDA’s non-medically related labeling. Therefore, doctors should not be branded with the additional duty of disclosing non-pertinent information, such as the FDA’s medically irrelevant distinction, to their patients
*It is estimated that 21% of all prescription drugs are prescribed “off-label.”
For fun, I took the countries that reportedly use Ivermectin country-wide and compared them to the USA, Israel and Sweden. I chose a three month cut-off, although the results were extended further. I did this because I don’t know when some of the countries began ivermectin use.
Can you guess who now has the highest death rates per million? Yeh –

12 Dec. 2021 – study in the city of Itajaí contains several methodological weaknesses, resulting in questionable conclusions
Oct. 4, 2021 – Brazil’s tragic ivermectin frenzy is a warning to the US, experts say
Read the article if you’re curious about what happened.
WHY WOULD YOU NOT USE EVERY AVAILABLE TREATMENT TO PREVENT PEOPLE FROM DYING.
WHY NOT?????????
TELL US WHY YOU ARE IRRATIONALLY SPREADING COVID DISINFORMATION BY SAYING THE VACCINE IS THE ONLY WAY TO PREVENT COVID DEATH?
WHY ARE YOU CUTTING OUT OTHER TREATMENTS WITH PATHETIC PROPAGANDA?
WHO’S GETTING PAID TO STOP SAVING AMERICAN LIVES?
HUNDREDS OF THOUSANDS OF PEOPLE HAVE DIED IN THIS COUNTRY BECAUSE TREATMENTS HAVE BEEN SUPPRESSED, AND A MARGINAL VACCINE HAS BEEN TOUTED AS BEING MORE EFFECTIVE THAN IT IS.
ANSWER ME!!!!
SO HOW MANY PEOPLE LIVED BECAUSE OF THIS “KIT?”
WHY ARE YOU SPREADING LIES TO GET PEOPLE TO STOP TRYING TO SAVE THEMSELVES FROM COVID???
THIS INSIDER “ARTICLE” IS COMPLETE GARBAGE BEREFT OF SCIENTIFIC RIGOR.
It’s propaganda that falls flat in the face of actual numbers.
You just don’t want people to take Ivermectin.
WHY????????
Just saying “it didn’t work” is not a viable statement.
How do you know it didn’t work?
Covid death is up in Israel, the most vaxxed nation.
By your logic, the vax didn’t work either.
Answer me!
Why wouldn’t you try Ivermectin? Why wouldn’t you try?
It’s FACT that is has saved at least one person.
There is real risk with the vaccine. It’s fact.
You can take both.
You can take one or the other.
You can take neither.
Why the f*ck is there a rabid moron here trying to get you not to take Ivermectin and MAKING you take the vaccine, NO questions asked?
Brazil spent less than $1 million on ALL the ivermectin the country bought.
Brazil only handed out a five-day treatment to some, not all, of their people in some, not all cities.
Too many people OD’ed after buying off poorer people’s kits and taking way too much.
Thus the high number of side effect sicknesses there.
Dr. Malone’s study shows what happens when people don’t take ivermectin, when they take only ten pills in 5 months (one course of two pills a day for 5 days after known exposure) and when people take 30 pills in 5 months (6 courses of two pills a day for 5 days.)
Notice the map of the world.
Brazil has the same SPORADIC ivermectin use as the USA.
And, here, ivermectin use is being throttled.
The doctors here won’t prescribe it.
The pharmacies won’t fill prescriptions for it.
The USPostal Service colludes with the FDA to prevent delivery of it from overseas by mail.
So, compare that throttling with Brazil’s same useage and see that your “study” (more propaganda than research) is nothing to be used for making an informed decision on.’
Saw my own doctor recently.
Sick as a dog after the 2nd, 3rd and 4th shots.
Told me she really hopes the CDC acts on the recommendation to allow a lot more time between shots.
The only tragedy in this is handing out medicine to people without a doctor’s prescription.
So the baked studies that confirm your bias and your agenda are right, and those that don’t are “questionable” or Rightwing propaganda?
That’s not how science and rational debate work, you clown.
Why wouldn’t you try Ivermectin? Why wouldn’t you try?
It’s FACT that is has saved at least one person.
There is real risk with the vaccine. It’s fact.
You can take both.
You can take one or the other.
You can take neither.
Why the f*ck is there a rabid moron here trying to get you not to take Ivermectin and MAKING you take the vaccine, NO questions asked?
Why wouldn’t you try Ivermectin? Why wouldn’t you try?
It’s FACT that is has saved at least one person.
There is real risk with the vaccine. It’s fact.
You can take both.
You can take one or the other.
You can take neither.
Why the f*ck is there a rabid moron here trying to get you not to take Ivermectin and MAKING you take the vaccine, NO questions asked?
It is ridiculous that an argument about an effective, cheap and available treatment and preventative has go on for so long. It will continue to go on because those who want to believe the least credible government in US history will believe that ivermectin is ineffective at best, dangerous at worst.
The argument is purely political. The argument against ivermectin is an argument in favor of government supremacy and control. An rancher with experience with treating animals with ivermectin, using the animal’s weight to calculate dosage, can and many have treated themselves. THAT’S how useful and benign the drug is. But those who think a totalitarian government would be best for us all want to deny the public the option of protection from the virus with cheap pharmaceuticals. Only the government knows what to do and the government says take a vaccine that is no longer effective against the variants. But… do it anyway, because that’s what the government says to do.
This is but one avenue of the politicization of the epidemic by Democrats that has killed people. Let’s go Brandon.