Not a single randomized controlled trial with verified outcome has been able to detect a statistically significant advantage of wearing a mask versus not wearing a mask, when it comes to preventing infectious viral illness
If there were any significant advantage to wearing a mask to reduce infection risk to either the wearer or others in the vicinity, then it would have been detected in at least one of these trials, yet there’s no sign of such a benefit
There is no evidence that masks are of any utility for preventing infection by either stopping the aerosol particles from coming out, or from going in. You’re not helping the people around you by wearing a mask, and you’re not helping yourself avoid the disease by wearing a mask
Infectious viral respiratory diseases primarily spread via very fine aerosol particles that are in suspension in the air. Any mask that allows you to breathe therefore allows for transmission of aerosolized viruses
All-cause mortality data are not affected by reporting bias. A detailed study of the current data of all-cause mortality shows the all-cause mortality this past winter was no different, statistically, from previous decades. COVID-19 is not a killer disease, and this pandemic has not brought anything out of the ordinary in terms of death toll
Denis Rancourt, Ph.D., a former full professor of physics, is a researcher with the Ontario Civil Liberties Association in Canada. He’s held that volunteer position since 2014, which has given him the opportunity to dig into scientific issues that impact civil rights. He also did postdoctoral work in chemistry.
Here, we discuss the controversial topic of face masks. Should you wear one? When and where? Does it protect you or not? There’s a wide range of opinions on this even within the natural health community.
Early on in the COVID-19 pandemic, I endorsed the use of face masks based on the experience of some of the Eastern European countries. The rationale of it seemed to make sense at the time. Since then, however, I’ve started to question their use.
Unfortunately, the mainstream propaganda and government orders in many states in recent weeks have reverted back toward mask wearing just about everywhere. You’re not allowed into stores; you cannot fly or take a cab, Uber or Lyft without one; you must wear one everywhere you go, even outdoors, and if you don’t you’re vilified, sometimes aggressively attacked.
There’s No Scientific Support for Mask-Wearing
Rancourt’s investigation into mask wearing was part of his research for the Ontario Civil Liberties Association. He did a thorough study of the scientific literature on masks, concentrating on evidence showing masks can reduce infection risk, especially viral respiratory diseases.
“What I found when I looked at all the randomized controlled trials with verified outcome, meaning you actually measure whether or not the person was infected … NONE of these well-designed studies that are intended to remove observational bias … found there was a statistically significant advantage of wearing a mask versus not wearing a mask.
Likewise, there was no detectable difference between respirators and surgical masks. That to me was a clear sign that the science was telling us they could not detect a positive utility of masks in this application.
We’re talking many really [high-]quality trials. What this means — and this is very important — is that if there was any significant advantage to wearing a mask to reduce this [infection] risk, then you would have detected that in at least one of these trials, [yet] there’s no sign of it.
That to me is a firm scientific conclusion: There is no evidence that masks are of any utility either preventing the aerosol particles from coming out or from going in. You’re not helping the people around you by wearing a mask, and you’re not helping yourself preventing the disease by wearing a mask.
This science is unambiguous in that such a positive effect cannot be detected. So, that was the first thing I publicized. I wrote a large review1,2 of the scientific literature about that.
But then I asked myself, as a physicist and as a scientist, why would that be? Why would masks not work at all? And so, I looked into the biology and physics of how these diseases are transmitted.”
The Importance of All-Cause Mortality Statistics
When trying to tease out whether an intervention works against COVID-19 or not, it’s important to look at death statistics. The number of deaths is really what’s important, not the number of infected individuals, as many may not even exhibit symptoms.
The problem is that assigning the cause of death in a situation where a viral infection taxes the immune system and is confounded by comorbidities is tricky business. As noted by Rancourt, epidemiologists have long known that you cannot reliably assign cause of death during a viral pandemic such as this. There’s tremendous bias involved.
To get around those problems, you have to look at all-cause mortality. The reason for this is because all-cause mortality data are not affected by reporting bias.
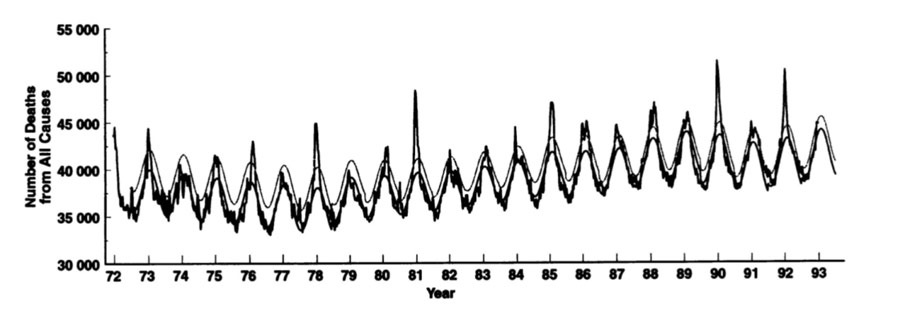
So, Rancourt did a detailed study of the current data of all-cause mortality, showing that the all-cause mortality this past winter was no different, statistically, from previous decades. In other words, COVID-19 is not a killer disease, and this pandemic has not brought anything out of the ordinary in terms of death toll.
Government Lockdown Orders Fueled Death Toll
He published this data in the paper,3 “All-Cause Mortality During COVID-19: No Plague and a Likely Signature of Mass Homicide by Government Response.” Rancourt explains:
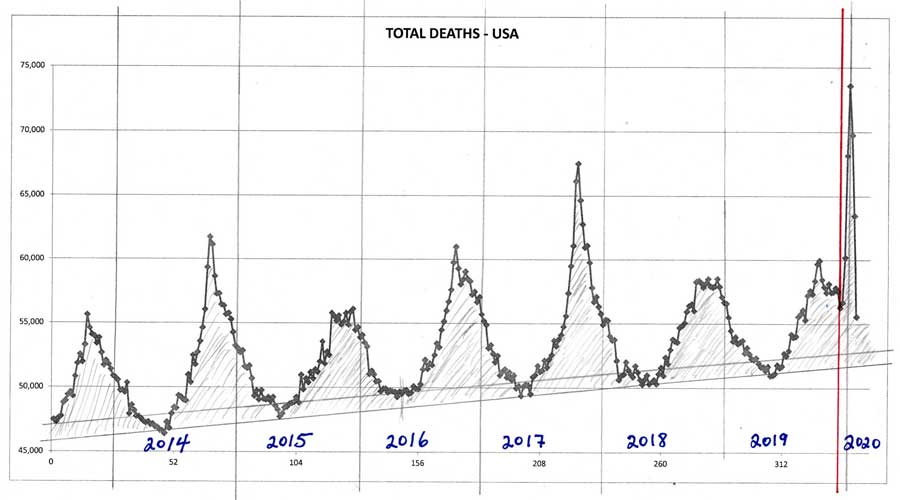
“It turns out that these curves, which show the winter burden deaths as humps every winter, some of them, in some jurisdictions, have an additional very sharp peak. It doesn’t represent a … huge amount of deaths by comparison to the total winter burden because it’s a very sharp peak, but it’s an anomalous peak. It’s not a natural peak.
And it happened in exact coincidence and time everywhere. In every jurisdiction that sees this anomalous, unnatural peak … the peak started exactly when the pandemic was declared by the World Health Organization. And the World Health Organization at that time recommended states prepare their hospitals for a huge influx of people with critical conditions.
So, the government response to that World Health Organization recommendation is what killed people, what accelerated the deaths. You can see that in the data, and you can also understand it in terms of how immune-vulnerable people are affected by these kinds of diseases.
What they did is they closed people into their institutional places of residence, they didn’t allow visitors. So, they isolated the most vulnerable parts of society that already had comorbidity conditions who were in a fragile state.
So, they ensured that many people that were locked into these institutions would die from this particular seasonal virus that causes the respiratory disease.
But the virus itself is not more virulent than other viruses. The total winter burden deaths is not greater, but there is a signature of a sharp feature that lasts the full width at half maximum. This feature is three or four or five weeks, which is extraordinarily rapid, never been seen before. And it happens very late in the winter burdens season.
A sharp peak like this has never been seen this late in the season before, and it’s happening [synchronistically] everywhere, on every continent, at the same time in direct immediacy after the declaration of the pandemic. To my eye, there is no doubt that there was an acceleration of deaths of vulnerable people due to government responses …
What really matters is the hard data, and the hard data is all-cause mortality in any jurisdiction that you want to look at. And it has not been anomalous, statistically speaking, no matter how you slice it.”
The two graphs below show the number of deaths from all causes from 1972 until 1993, and 2014 until present time in 2020.
Why Government Response Was Ill Advised
Rancourt goes on to qualify some of this data based on the mechanism of viral transmission, which also helps explain why government responses have been ill advised, as they actually worsen transmission rather than inhibit it. Infectious respiratory diseases primarily spread via very fine aerosol particles that are in suspension in the air.
“We’re talking about the small size fraction of aerosols, so typically smaller than 2 micrometers,” Rancourt explains. “There are water droplets that bear these virions, the virus particles, and there can be dozens or hundreds of these virions per very small droplet of this size.
Those are the droplets we’re talking about. When you get down to those sizes, gravitational outtake is very inefficient and they basically stay in suspension. And, as soon as you have currents or flow of air, [the particles] are carried.”
The aerosol particles stay in suspension when the absolute humidity is low. This is why influenza outbreaks occur during the winter. Once absolute humidity rises, the aerosol particles become unstable. They agglomerate, drop out of suspension and cease to be transmissible. “This is well known,” Rancourt says. “It’s been known for a decade. It’s been extraordinarily well-demonstrated by top scientists.”
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
Connect with
I allow to create an account
When you login first time using a Social Login button, we collect your account public profile information shared by Social Login provider, based on your privacy settings. We also get your email address to automatically create an account for you in our website. Once your account is created, you'll be logged-in to this account.
DisagreeAgree
35 Comments
Inline Feedbacks
View all comments
kitt
3 years ago
But the consensus no damn proof science, where a cleaned or disinfected area has less infection is no longer valid just put on the damn mask cause it proves we can control the narrative and you.
Nan G
3 years ago
Seems you can find doctors who will say anything.
This AM Fox Business had a doctor on who often wishes it were not protocol to wear a mask during surgery!
If it were not a requirement he would not wear one even then!
We built a 2 dozen double cloth masks with pockets for an antiviral tissue to fit inside.
I think I posted the How-To video here earlier.
Utah’s businesses are requiring masks even if the state, county or city does not.
So, you end up needing to have a clean one with you anyway.
Might as well be one that has a best chance of helping.
Still the distancing and the staying home more has probably helped as much as the masks.
At my age I just hope to not catch it until a vaccine is available, or an agreed upon treatment that really works.
Greg
3 years ago
The article is dangerous nonsense. The studies involved the effectiveness of masks in reducing transmission of colds and influenza, which are mainly spread through direct hand contact with virus-contaminated surfaces, and then touching the eyes, nose, or mouth. Evidence strongly indicates that COVID-19 is mainly contracted by inhaling contaminated droplets that have been exhaled by an infected person in the immediate vicinity of an uninfected person.
Why encourage people to put themselves and other at greater risk, when experts believe several weeks of widespread mask use could bring the pandemic under control? Why increase the risks to businesses and the national economy? What’s the point?
Deplorable Me
3 years ago
Since the beginning of this epidemic, I have gone out, to the store or whatever, and not worn a mask unless it was mandated. Only recently has it been mandated in stores and restaurants, and then only when social distancing cannot be maintained or upon entering or leaving a restaurant. My wife and I just recently drove to Corpus Christi and spent 4 days for our 45th wedding anniversary. Last Wednesday, after we returned, I gave blood. They do an antibodies test.
I don’t have and have not had COVID19. That pretty much indicates my wife is clear as well. It’s not that difficult to avoid catching it.
kitt
3 years ago
@Greg: You failed to read the article if you can breathe the tiny microscopic virus particles are passing right through the mask. Both directions inhale the virus exhale the virus.
I know you dont believe the science of invisible germs, the whole thing is a curse from the Angry god Hillary sacrifices chickens to with Mills in her back yard.
The virus doesn’t fly around in the air on tiny little wings. It’s carried on moisture droplets that are produced when people exhale, talk, cough, or sneeze. The droplets are vastly larger than the COVID-19 virus that can contaminate them. The droplets can be caught when they pass through the fibers of a mask. If the droplets stick to the mask fibers, that reduces the likelihood that the virus that they carry will wind up in an uninfected person’s lungs. Less likelihood means less overall transmission.
kitt
3 years ago
@Greg: Infectious respiratory diseases primarily spread via very fine aerosol particles that are in suspension in the air. They pass through the mask with every breath. Blast through with a cough or sneeze. They are teeny teeny teeny tiny which is why in an infectious disease lab they wear those space suit looking outfits and not just masks.
Your logic and information are faulty. Your cheap China masks are no protection.
Greg
3 years ago
More people will die and more businesses will fail if people refuse to adopt a simple and effective measure that’s little more than a minor inconvenience. That’s what logic should be telling people. It’s not rocket science. It’s easy to figure out. Or it should be.
Do you really believe that a simple cloth mask doesn’t catch a lot of projected droplets with a person coughs or sneezes?
kitt
3 years ago
@Greg: People are always suppose to cough into their elbow or sneeze into a tissue who the hell doesnt?
News flash there are currently 6 known mutations all with varying levels of severity.
People die but .04% from covid19, it isnt a death sentence never has been a death sentence, get a grip. this no longer qualifies as an epidemic.
More people will die and more businesses will fail if people refuse to adopt a simple and effective measure that’s little more than a minor inconvenience.
But massed protests and riots EVERY NIGHT is OK?
Jim
3 years ago
@Greg: I hope you die a slow, miserable, painful death from covid, you commie asshole. They can bury you with your mask.
Do you really believe that a simple cloth mask doesn’t catch a lot of projected droplets with a person coughs or sneezes?
While I think you have a partisan agenda and you are basically a disinformation douche bag, I do agree…it’s very hard for me not to believe that the masks help…
As far as the article above, I just don’t buy it.
I have worn a mask from the beginning for two reasons: 1) To mitigate even the slightest chance I spread the disease, and 2) As and act of solidarity that I’m taking the virus seriously.
I agree with people having the right not to wear one, and I think Trump and Biden shouldn’t have to wear one at the podium or anywhere if they can do it safely.
While I think you have a partisan agenda and you are basically a disinformation douche bag, I do agree…it’s very hard for me not to believe that the masks help…
You know, first, leftists like Greg have to create the false argument that Trump opposes wearing masks. He doesn’t. Then they have to invent the argument that masks are absolutely necessary 100% of the time.
Ronald J. Ward
3 years ago
Trump said today that wearing masks were patriotic, even Tweeting a pic of him in a mask.
So you know what that means, right?
It means now you must, as solid Trump supporting mindless sheep, now defend the mask, encourage the mask, even put one one your very Trump ass sucking faces.
How about maybe getting some Trump ass scent to put on them to make you feel better?
Deplorable Me
3 years ago
@Ronald J. Ward: Your fantasy of a swarm of people denouncing masks is just that; a false fantasy created by left wing liars. Trump never opposed masks; it is simply that they are not necessary 100% of the time, are not the cure-all and not objected to in reasonable conditions.
The mask is very breathable and does not cause breathing pressure
The reason being that this mask is, indeed, utterly useless.
Randy
3 years ago
@Greg: I let this sit for a while hoping that greggie the rock would finally understand how viruses really move from people to people. There is plenty of references out there. First, the article is right. The masks are useless and likely cause more harm to the user. Viruses do go through the masks to include surgical masks. The virus is carried on water droplets that first impact on the inside of the mask. The mask gets wet from continuous use and the virus moves through the mask and is aerosolized on the outside of the mask and sent back into the air. Surgical masks are primarily used to guard against bacterial contamination of the patient since bacterial infections are most prominent in surgery.
The most stringent standard for masks is ATSM with a 98% efficiency at .1 microns. NIOSH is 98% at .3 microns. Virus size is .3 to .005 micron. Bacterial size is .3 microns to 60 microns. Viruses are carried in water droplets that impact on the inside of the mask. The virus is deposited there, too. With continuous use, the virus is pushed through the pores of the mask and inserted into water droplets on the outside of the mask. These droplets containing the virus is then propelled forward although not as high a velocity as inside of the mask. The fit of the mask on the face also determines the effectiveness of the mask. If your glasses fog up when you breath, you mask is useless. Also, if there is air escaping along the sides, it is also useless. If you use a high density of mask that may reach the .1 micron size, the less air is filtered and more escapes or enters along the sides. Of the masks tested by NIOSH, who certifies masks/respirators, 80-nearly 100% failed the NIOSH criteria of 98% at .3 micron. The Corona virus is .06 to .14 microns in size. Also another note. Surgical masks of the highest efficiencies are single use, not single use for a day. A surgeon is likely to go through several masks during surgery. How many people use several masks per day. Because they do not, the masks harbor the virus and also propagates dangerous bacteria in the moist environment. The best use of masks is to give those who wear them a false sense of security.
Greg
3 years ago
How many times must it be pointed out that the size of the virus is totally irrelevant?
Masks significantly reduce expelled droplets that get into the air.
The COVID-19 virus travels through the air on expelled droplets.
Therefore, simple masks reduce the likelihood of transmission and exposure.
greggie the rock, what is being denied is your logic and that of people who want to pretend to be experts. Show me a study that shows proof how viruses react when people are wearing masks. There is only theories. Also greggie the rock, Viruses are not only carried on water droplets. The may start out that way, but what happens when the water evaporates? What happens when someone wears the same mask all day or for many days? Are there water droplets on all of the surfaces that have been sampled and viruses have been found? No! NIOSH has determined that the best surgical masks do not meet their standards for retaining viruses, yet you know it all!
NIOSH has determined that the best surgical masks do not meet their standards for retaining viruses, yet you know it all!
No one said that they did. Total protection for a worker handling deadly infectious microorganisms would require a positive pressure isolation suit.
They DID NOT say that simple masks are useless in significantly reducing the spread of COVID-19. Nor will they, because it isn’t true. Simple masks significantly reduce the likelihood of transmission.
The Governor of Indiana, a staunch Republican and conservative, has today mandated the wearing of masks in all indoor public places, and in outdoor public places where social distancing cannot be done, effective July 27. The reason is because COVID-19 is on the rise again following Indiana’s measured reopening, and because all experts agree that masks are one of the simplest measures that can effectively protect Indiana’s citizens, businesses, and economy.
Governor Holcomb is certainly not doing this for political reasons. He knows perfectly well that the decision isn’t widely popular in a strongly republican state. He’s putting reason and the good of the population ahead of popularity and politics, and I applaud him for that.
kitt
3 years ago
@Randy: Not that larger droplets dont become smaller droplets as they evaporate carrying the virus with them through the fibers. As one has to inhale deeper to get the same amt of oxygen you suck them right in or exhale the finer mist right out.
These people are liars and faking numbers of infected
Brock Ballou (cool name) told cowboy town’s News4 he’d been expecting a contact tracer call, given that a coworker had tested positive for the Wuhan flu.
But he got a surprise:
“She specifically said – I’m looking at it right here – you tested positive – this is a follow up call to see how your symptoms are.” The guy had never even taken a test.
WSMV asked Brock — was he certain he heard her correctly?
Yep:
“I’m 100 percent sure that’s what she said, she was looking right at it. She told me I’m in the system – ‘looking right at it that you’re showing positive.’”
Was it a prank? Not according to the station — it claims to have confirmed that all three phone numbers from Brock’s incoming COVID confusion were indeed from the Tennessee Department of Health.
They got his name through contact tracing, never tested but reported in the positive numbers.
a spokeswoman clarified she’s not worried about accuracy:
“I can also tell you there is no concern with our count of cases in regard to our reporting of those who test positive. Those entries are based on lab results, not on information provided from the monitoring team.” Further he was told it was a 3rd party contractor..lies the calls came from their office.
Simple masks significantly reduce the likelihood of transmission.
Show one study that proves this! There isn’t one which is why CDC initially advised against wearing masks. You really do not know what you are talking about greggie the rock. I have been recommending and single use masks and respirators for over 40 years to provide protection against biologicals as well as particulates. Only air supplied respirators work on viruses. Go to ATSM and NIOSH if you want to learn something. Then get certified in fitting respirators that meet federal law. Also, did you think about all of the bacteria that is now caught in the masks and allowed to multiply? One of the big issues with the Corona virus infection is bacterial pneumonia. That is why part of the treatment is antibiotics.
Governor Holcomb is certainly not doing this for political reasons. He knows perfectly well that the decision isn’t widely popular in a strongly republican state.
Yes he is. He and all of the resisters are blaming Trump. Stick to something that you know something about greggie the rock. You may continue this line of thought and show you the extent of your ignorance.
@Greg: Too bad he didn’t know he had it and didn’t cough in the fat tub of shit Nadler’s face. How many co-morbidities does that waste of flab have, do you think?
Gomert will get on a quick regimen of hydroxychloroquine and be over this in no time.
Nan G
3 years ago
@Greg: Actually, Greg, what he said was that his personal habit of touching his mask to adjust it was probably a contributor to his getting infected.
All health experts agree that this is a risk when it comes to non-experts wearing masks.
It is really hard to keep one’s fingers off of them.
Greg
3 years ago
I’ve been taking the increasing hostility of Trump supporters as an indication that a few unwelcome truths might be slowly sinking in.
Gohmert suggests without evidence that wearing mask contributed to contracting coronavirus
Seriously suggested did not state as a fact but he must have evidence, what a pile of pony poo. His mask could have had cross contamination from any source. You know how you got VD buddy from a toilet seat. I did notice Nadler fondling his mask with his filthy dirty germy hands cause he couldnt properly get the elastic over his fat head.
Deplorable Me
3 years ago
@Greg: No, we are merely fed up with the left wing violence and desperation.
Greg
3 years ago
I thought it would be hard to top Gohmert’s public speculation that he might have caught COVID-19 from his mask. I should have known better. This guy didn’t even allow a decent interval before working up an exploitable angle.
Deplorable Me
3 years ago
@Greg: Well, do masks work or do we need goggles now?
kitt
3 years ago
@Deplorable Me:Fauchis little CYA for his lying cause masks have never worked, its about Hygiene. We know Californias Mask order did nothing to slow the spread.
Deplorable Me
3 years ago
@kitt: Or China, Japan or the Koreas, where they are used to wearing masks.
…to make no mention of numerous unidentified Secret Service personnel, Trump’s advance rally organizers, and military personnel assigned to his presidential aircraft.
Deplorable Me
3 years ago
@Greg: Pelosi just introduced a mask policy. Apparently, when the cameras weren’t on, it wasn’t that important to that drunken skank.



But the consensus no damn proof science, where a cleaned or disinfected area has less infection is no longer valid just put on the damn mask cause it proves we can control the narrative and you.
Seems you can find doctors who will say anything.
This AM Fox Business had a doctor on who often wishes it were not protocol to wear a mask during surgery!
If it were not a requirement he would not wear one even then!
We built a 2 dozen double cloth masks with pockets for an antiviral tissue to fit inside.
I think I posted the How-To video here earlier.
Utah’s businesses are requiring masks even if the state, county or city does not.
So, you end up needing to have a clean one with you anyway.
Might as well be one that has a best chance of helping.
Still the distancing and the staying home more has probably helped as much as the masks.
At my age I just hope to not catch it until a vaccine is available, or an agreed upon treatment that really works.
The article is dangerous nonsense. The studies involved the effectiveness of masks in reducing transmission of colds and influenza, which are mainly spread through direct hand contact with virus-contaminated surfaces, and then touching the eyes, nose, or mouth. Evidence strongly indicates that COVID-19 is mainly contracted by inhaling contaminated droplets that have been exhaled by an infected person in the immediate vicinity of an uninfected person.
Why encourage people to put themselves and other at greater risk, when experts believe several weeks of widespread mask use could bring the pandemic under control? Why increase the risks to businesses and the national economy? What’s the point?
Since the beginning of this epidemic, I have gone out, to the store or whatever, and not worn a mask unless it was mandated. Only recently has it been mandated in stores and restaurants, and then only when social distancing cannot be maintained or upon entering or leaving a restaurant. My wife and I just recently drove to Corpus Christi and spent 4 days for our 45th wedding anniversary. Last Wednesday, after we returned, I gave blood. They do an antibodies test.
I don’t have and have not had COVID19. That pretty much indicates my wife is clear as well. It’s not that difficult to avoid catching it.
@Greg: You failed to read the article if you can breathe the tiny microscopic virus particles are passing right through the mask. Both directions inhale the virus exhale the virus.
I know you dont believe the science of invisible germs, the whole thing is a curse from the Angry god Hillary sacrifices chickens to with Mills in her back yard.
@kitt, #5:
The virus doesn’t fly around in the air on tiny little wings. It’s carried on moisture droplets that are produced when people exhale, talk, cough, or sneeze. The droplets are vastly larger than the COVID-19 virus that can contaminate them. The droplets can be caught when they pass through the fibers of a mask. If the droplets stick to the mask fibers, that reduces the likelihood that the virus that they carry will wind up in an uninfected person’s lungs. Less likelihood means less overall transmission.
@Greg: Infectious respiratory diseases primarily spread via very fine aerosol particles that are in suspension in the air. They pass through the mask with every breath. Blast through with a cough or sneeze. They are teeny teeny teeny tiny which is why in an infectious disease lab they wear those space suit looking outfits and not just masks.
Your logic and information are faulty. Your cheap China masks are no protection.
More people will die and more businesses will fail if people refuse to adopt a simple and effective measure that’s little more than a minor inconvenience. That’s what logic should be telling people. It’s not rocket science. It’s easy to figure out. Or it should be.
Do you really believe that a simple cloth mask doesn’t catch a lot of projected droplets with a person coughs or sneezes?
@Greg: People are always suppose to cough into their elbow or sneeze into a tissue who the hell doesnt?
News flash there are currently 6 known mutations all with varying levels of severity.
People die but .04% from covid19, it isnt a death sentence never has been a death sentence, get a grip. this no longer qualifies as an epidemic.
@Greg:
But massed protests and riots EVERY NIGHT is OK?
@Greg: I hope you die a slow, miserable, painful death from covid, you commie asshole. They can bury you with your mask.
@Jim:
Greg Nye the science guy.
@Greg:
While I think you have a partisan agenda and you are basically a disinformation douche bag, I do agree…it’s very hard for me not to believe that the masks help…
As far as the article above, I just don’t buy it.
I have worn a mask from the beginning for two reasons: 1) To mitigate even the slightest chance I spread the disease, and 2) As and act of solidarity that I’m taking the virus seriously.
I agree with people having the right not to wear one, and I think Trump and Biden shouldn’t have to wear one at the podium or anywhere if they can do it safely.
@Nathan Blue:
You know, first, leftists like Greg have to create the false argument that Trump opposes wearing masks. He doesn’t. Then they have to invent the argument that masks are absolutely necessary 100% of the time.
Trump said today that wearing masks were patriotic, even Tweeting a pic of him in a mask.
So you know what that means, right?
It means now you must, as solid Trump supporting mindless sheep, now defend the mask, encourage the mask, even put one one your very Trump ass sucking faces.
How about maybe getting some Trump ass scent to put on them to make you feel better?
@Ronald J. Ward: Your fantasy of a swarm of people denouncing masks is just that; a false fantasy created by left wing liars. Trump never opposed masks; it is simply that they are not necessary 100% of the time, are not the cure-all and not objected to in reasonable conditions.
For the fashion-conscious girl who just doesn’t get it, but wants to pretend that she does…
A 5-star product review:
The reason being that this mask is, indeed, utterly useless.
@Greg: I let this sit for a while hoping that greggie the rock would finally understand how viruses really move from people to people. There is plenty of references out there. First, the article is right. The masks are useless and likely cause more harm to the user. Viruses do go through the masks to include surgical masks. The virus is carried on water droplets that first impact on the inside of the mask. The mask gets wet from continuous use and the virus moves through the mask and is aerosolized on the outside of the mask and sent back into the air. Surgical masks are primarily used to guard against bacterial contamination of the patient since bacterial infections are most prominent in surgery.
The most stringent standard for masks is ATSM with a 98% efficiency at .1 microns. NIOSH is 98% at .3 microns. Virus size is .3 to .005 micron. Bacterial size is .3 microns to 60 microns. Viruses are carried in water droplets that impact on the inside of the mask. The virus is deposited there, too. With continuous use, the virus is pushed through the pores of the mask and inserted into water droplets on the outside of the mask. These droplets containing the virus is then propelled forward although not as high a velocity as inside of the mask. The fit of the mask on the face also determines the effectiveness of the mask. If your glasses fog up when you breath, you mask is useless. Also, if there is air escaping along the sides, it is also useless. If you use a high density of mask that may reach the .1 micron size, the less air is filtered and more escapes or enters along the sides. Of the masks tested by NIOSH, who certifies masks/respirators, 80-nearly 100% failed the NIOSH criteria of 98% at .3 micron. The Corona virus is .06 to .14 microns in size. Also another note. Surgical masks of the highest efficiencies are single use, not single use for a day. A surgeon is likely to go through several masks during surgery. How many people use several masks per day. Because they do not, the masks harbor the virus and also propagates dangerous bacteria in the moist environment. The best use of masks is to give those who wear them a false sense of security.
How many times must it be pointed out that the size of the virus is totally irrelevant?
Masks significantly reduce expelled droplets that get into the air.
The COVID-19 virus travels through the air on expelled droplets.
Therefore, simple masks reduce the likelihood of transmission and exposure.
What is being denied is logic.
@Greg:
greggie the rock, what is being denied is your logic and that of people who want to pretend to be experts. Show me a study that shows proof how viruses react when people are wearing masks. There is only theories. Also greggie the rock, Viruses are not only carried on water droplets. The may start out that way, but what happens when the water evaporates? What happens when someone wears the same mask all day or for many days? Are there water droplets on all of the surfaces that have been sampled and viruses have been found? No! NIOSH has determined that the best surgical masks do not meet their standards for retaining viruses, yet you know it all!
@Randy, #20:
No one said that they did. Total protection for a worker handling deadly infectious microorganisms would require a positive pressure isolation suit.
They DID NOT say that simple masks are useless in significantly reducing the spread of COVID-19. Nor will they, because it isn’t true. Simple masks significantly reduce the likelihood of transmission.
The Governor of Indiana, a staunch Republican and conservative, has today mandated the wearing of masks in all indoor public places, and in outdoor public places where social distancing cannot be done, effective July 27. The reason is because COVID-19 is on the rise again following Indiana’s measured reopening, and because all experts agree that masks are one of the simplest measures that can effectively protect Indiana’s citizens, businesses, and economy.
Governor Holcomb is certainly not doing this for political reasons. He knows perfectly well that the decision isn’t widely popular in a strongly republican state. He’s putting reason and the good of the population ahead of popularity and politics, and I applaud him for that.
@Randy: Not that larger droplets dont become smaller droplets as they evaporate carrying the virus with them through the fibers. As one has to inhale deeper to get the same amt of oxygen you suck them right in or exhale the finer mist right out.
These people are liars and faking numbers of infected
Brock Ballou (cool name) told cowboy town’s News4 he’d been expecting a contact tracer call, given that a coworker had tested positive for the Wuhan flu.
But he got a surprise:
“She specifically said – I’m looking at it right here – you tested positive – this is a follow up call to see how your symptoms are.”
The guy had never even taken a test.
WSMV asked Brock — was he certain he heard her correctly?
Yep:
“I’m 100 percent sure that’s what she said, she was looking right at it. She told me I’m in the system – ‘looking right at it that you’re showing positive.’”
Was it a prank? Not according to the station — it claims to have confirmed that all three phone numbers from Brock’s incoming COVID confusion were indeed from the Tennessee Department of Health.
They got his name through contact tracing, never tested but reported in the positive numbers.
a spokeswoman clarified she’s not worried about accuracy:
“I can also tell you there is no concern with our count of cases in regard to our reporting of those who test positive. Those entries are based on lab results, not on information provided from the monitoring team.” Further he was told it was a 3rd party contractor..lies the calls came from their office.
@Greg:
Show one study that proves this! There isn’t one which is why CDC initially advised against wearing masks. You really do not know what you are talking about greggie the rock. I have been recommending and single use masks and respirators for over 40 years to provide protection against biologicals as well as particulates. Only air supplied respirators work on viruses. Go to ATSM and NIOSH if you want to learn something. Then get certified in fitting respirators that meet federal law. Also, did you think about all of the bacteria that is now caught in the masks and allowed to multiply? One of the big issues with the Corona virus infection is bacterial pneumonia. That is why part of the treatment is antibiotics.
Yes he is. He and all of the resisters are blaming Trump. Stick to something that you know something about greggie the rock. You may continue this line of thought and show you the extent of your ignorance.
From FOX News, July 29, 2020 – Rep Gohmert tests positive for coronavirus ahead of Texas visit with Trump
There’s no cure for stupid:
Gohmert suggests without evidence that wearing mask contributed to contracting coronavirus
@Greg: Too bad he didn’t know he had it and didn’t cough in the fat tub of shit Nadler’s face. How many co-morbidities does that waste of flab have, do you think?
Gomert will get on a quick regimen of hydroxychloroquine and be over this in no time.
@Greg: Actually, Greg, what he said was that his personal habit of touching his mask to adjust it was probably a contributor to his getting infected.
All health experts agree that this is a risk when it comes to non-experts wearing masks.
It is really hard to keep one’s fingers off of them.
I’ve been taking the increasing hostility of Trump supporters as an indication that a few unwelcome truths might be slowly sinking in.
@Greg:
Seriously suggested did not state as a fact but he must have evidence, what a pile of pony poo. His mask could have had cross contamination from any source. You know how you got VD buddy from a toilet seat. I did notice Nadler fondling his mask with his filthy dirty germy hands cause he couldnt properly get the elastic over his fat head.
@Greg: No, we are merely fed up with the left wing violence and desperation.
I thought it would be hard to top Gohmert’s public speculation that he might have caught COVID-19 from his mask. I should have known better. This guy didn’t even allow a decent interval before working up an exploitable angle.
@Greg: Well, do masks work or do we need goggles now?
@Deplorable Me:Fauchis little CYA for his lying cause masks have never worked, its about Hygiene. We know Californias Mask order did nothing to slow the spread.
@kitt: Or China, Japan or the Koreas, where they are used to wearing masks.
GOP congressional staffers have reported being pressured not to wear masks.
Herman Cain might still be alive, if he’d done so. He attended Trump’s Tulsa rally unmasked.
Gohmert is positive—and still talking down masks.
A look at White House aides, campaign staff who have tested positive for coronavirus
…to make no mention of numerous unidentified Secret Service personnel, Trump’s advance rally organizers, and military personnel assigned to his presidential aircraft.
@Greg: Pelosi just introduced a mask policy. Apparently, when the cameras weren’t on, it wasn’t that important to that drunken skank.