
![]()
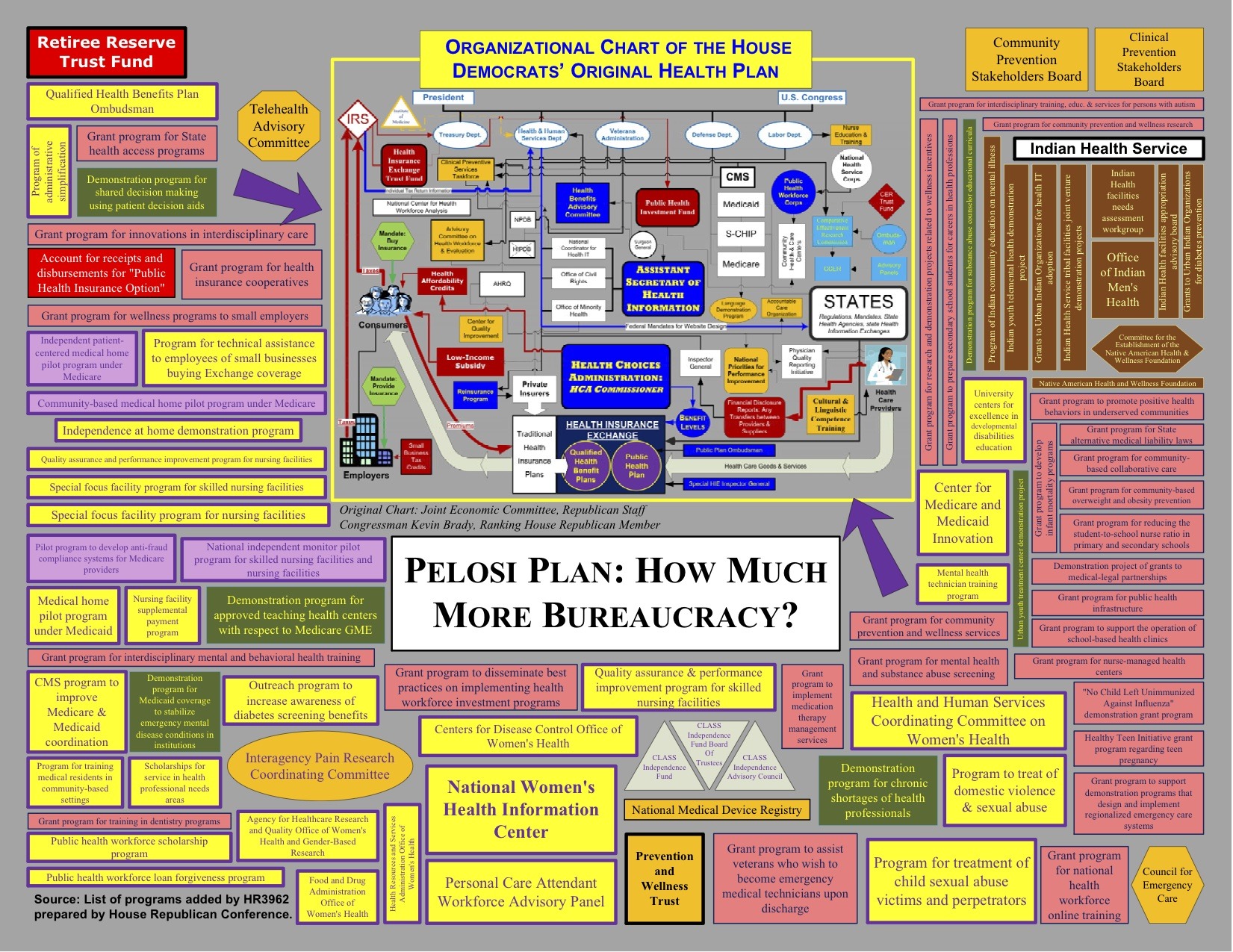
Tom Blumer from BizzyBlog has updated his map of the ObamaCare/PelosiCare behemoth and what it creates. Namely 111 agencies, regulators, committees, boards and offices: (click on picture to enlarge)
Meanwhile Senator Gregg reacts to the new CBO estimate:
Senator Judd Gregg (R-NH), ranking member of the Senate Budget Committee today commented on the Congressional Budget Office’s (CBO) more detailed cost estimate of the manager’s amendment to the House health reform bill.
Senator Gregg stated, “The CBO estimate released last night finally sheds light on the smoke and mirrors game the majority has been playing with the cost of their health care reform proposal. Over the first 10 years, this legislation builds in gross new spending of $1.7 trillion – and most of the new spending doesn’t even start until 2014. Once that spending is fully phased in, the House Democratic bill rings up at more than $3 trillion over ten years.
“Additionally, this bill cuts critical Medicare and Medicaid funding by $628 billion, accounts for nearly $1.2 trillion in tax and fee increases and will explode the scope of government by putting the nation’s health care system in the hands of Washington bureaucrats. The $3 trillion price tag defies common sense – we simply cannot add all this new spending to the government rolls and claim to control the deficit.
“If we continue to pile more and more debt on the next generation, they will never be able to get out from under it. The health care system needs reform, but this massive expansion of government, financed by our children and grandchildren, is the wrong way to proceed.”
And listen…this is what our government believes will be the cost. But look at programs our government has run historically and you find decades of added costs and overruns that our forced onto the taxpayer.
Insanity

See author page

@mata (#160): There’s nothing tremendously wrong with IMAC, as proposed in the language of the document you linked. They are just setting broad reimbursement formulas for major classes of procedures. They are not doing detailed adjustment of individual drugs, operations, diagnostic tests, etc. They are not deciding which patients get treated and which don’t. They are a mixed panel of experts, from both political parties. They are very analogous to the Federal Reserve, only they are accountable to both President and the Senate. They are certainly nothing like a death panel. Neither is anything relating to the end of life counseling stuff, as we’ve discussed previously.
If IMAC, the President, and the Senate set reimbursements too low, providers will drop out and they’ll have to increase levels.
As I wrote, the GOP screams that Medicare is failing; George Bush only made the Medicare problem worse. Obama is trying to fix Medicare, so that it will be available for all of us, and Palin and her supporters scream “death panels.” Which is despicable scaremongering by despicable people.
I never accused you of being one of those screaming “death panels.” I do argue stridently against the people who did that and against those who defend them for screaming “death panels.”
You can moralize or you can try to fix a very big problem. You think that doctors in private practice should be paid for doing surgery and pushing poisons and directing ray guns but not paid for counseling, which is, in the situations we are discussing, far more efficacious, to say nothing of far more humane. You expect altruistic standards of doctors which are found nowhere else in capitalist society, and, when those standards are not met, you support those scaremongering with accusations of “death panels,” as opposed to those who try to come up with real world solutions to previously-intractable problems.
How do you propose to encourage more counseling and less ineffective treatment? Threaten physicians with incarceration?
It’s good legislation which was killed by “Pants on Fire,” lying scaremongering.
– Larry Weisenthal/Huntington Beach, CA
Nothing earth shaking here Larry.
One would have to be living under a rock not to recognize that the ‘ current’ GOP could give a crap about social issues, especially abortion. They “tolerate” and “talk the talk” for the simple reason they can’t win without the social conservatives. If they could win without us, we would be “under the bus” in no time.
On the other hand, many of them feel secure in their “big tent” theory, assuming the social conservatives have no where else to go. I predict Sarah Palin will change that, and continue my prediction from a year ago that if Palin runs for POTUS, it will NOT be with the GOP.
Abortion is a CONSERVATIVE issue, not to be confused with the GOP.
Larry, all you really keep saying is it’s for our own good.
Mata, thank you for taking the time to show how wrong larry is. Your knowledge of the proposals is very impressive.
@ Hard Right
What Mata has provided in this regard, is nothing short of breathtaking.
Patvann, for once I didn’t want to needle larry. Since you did, I MUST agree. Breathtaking indeed.
And what would you describe the Hippocratic Oath as but altruistic?
In case you don’t remember, Larry… the text of the Hippocratic Oath from the Harvard Classics translation
hummmm… I wonder if those evil Wall Street CEOs have a similar oath
BTW, Larry… I want you to ponder your statement below carefully, and let us all know how it differs from Palin’s comment that such counsel is a subtle encouragement to end your life earlier in order to save government costs:
For a brief scroll refresher course, let’s compare that with what Palin quoted Eugene Robinson (o’healthcare supporter) said… where that “scaremonger”, “despicable” Palin thoroughly agreed. Again, from her testimony text:
So… this “scaremongering” differs from your statement HOW?
Mata good luck with the Hippocratic Oath argument. Most MD’s never even take it anymore.
Between Ezechiel Emanual on record of “we take it too seriously”, to the Julie Cantor’s (MD, JD) op-ed in the NEJM advising any physician who has a problem with “anything legal” to best go into podiatry, it’s a mute point, gone the way with our moral decline.
Cantor’s rant was more focused on the Bush Conscience clause but in the end, all one in the same.
Touche’ Mata…… you called that one dead on!!!
Seems too many times it’s not WHAT was said …..as opposed to WHO said it!!
@Mata:
#167,168:
Here’s the difference, Mata:
Here’s what Palin said:
This is scaremongering. What I wrote was factual, sensible, and not scaremongering. With respect to Mr. Robinson, what he was pointing out was the need to educate the public. Remember, the “dialogue” which was supposed to take place at those Town Hall meetings where, instead, the Senators and Representatives who came their to explain the legislation and answer questions were, instead, shouted down by citizens whipped into a frenzy by Palin’s irresponsible and dishonest scaremongering.
Regarding my quote (above): There are two huge problems, which are related to each other.
The first problem is runaway, unsustainable health care costs. 16% of GDP, headed up to 33% of GDP. Small business (“the engine of the economy”) health insurance premiums rising this year by 15%, at a time when there’s 11% unemployment and virtually no inflation in the rest of the economy. Medicare on a path to insolvency. Somewhere between 25 and 30% of Medicare expenses are for patients in the last year of life. Half of all people surveyed say that, were they to have a chronic, terminal illness, they’d prefer to die at home, rather than in the hospital.
http://content.healthaffairs.org/cgi/reprint/20/4/188.pdf
Hospice care is often the choice of patients and families, when the patients can no longer be cared for at home. Hospice isn’t a one way street for poor people who can’t afford private duty nurses at home. Art Buchwald entered a hospice, stayed there 5 months, and then left, when his kidney failure stabilized.
However, all of the financial incentives today in medicine are for performing diagnostic tests and providing active treatments, even in the frequent situations (e.g. terminal cancer) where treatments are toxic and more likely to hurt than to help.
So you’ve got a situation which cries out for reform. The reform proposed was simple and humane. Pay doctors for counseling patients, as doctors are currently paid for treating patients. The amount of money that doctors would get for counseling would still be a fraction of what they’d get for treating, but it would be at least something, and I believe that it would lead to more counseling.
I’ve explained the “rules” of the counseling previously and I’ve explained how you were not correct to claim that this counseling was ever intended to be “mandatory” or that it could ever be possibly construed to be “mandatory” by anyone familiar with Medicare reimbursement rules.
With regard to the Hippocratic OathL
You don’t understand this any better than you understood the proposed legislation regarding end of life counseling:
Mata, the above quote says this:
“him who taught me this art” refers to one’s mentors and professors. One is obligated to provide all necessary care to one’s mentor (the person who was the teacher to said doctor) and to teach the offspring of one’s mentor the art of medicine, should said offspring wish to learn it. And such teaching must be provided without fee or stipulation, meaning that I am supposed to train my mentor’s children in the art of medicine without charging them tuition. Furthermore (it continues) I promise to train my own sons in the Art of medicine as well as the sons of my teachers, and to other students who agree to be bound by the law of medicine, but not to train students who do not agree to be bound by the “law of medicine.”
The above says nothing at all about providing medical services without compensation; it only says that must agree to train the sons of their own mentors “without fee or stipulation.” Would that this were true today; I’ve trained a fair number of medical students and interns and residents and fellows, who today are excellent physicians. It would be nice if they would agree to train my own offspring for free, to spare the necessity of paying $45,000 per year in tuition and fees.
Continuing:
Yes. Hear hear. But here’s the rub (following is a quote often cited by oncologists):
One can almost always justify pushing more chemotherapy. Or even doing another surgery or radiation treatment. I saw an interesting study presented at the recent (October) American Society of Clinical Oncology breast cancer meetings in San Francisco. They did a survey of patients and oncologists and asked each group how long a life prolongation would be required to make chemotherapy “worth it.” It was quite interesting. The large majority of oncologists felt that a 2-4 month life prolongation was “worth it.” More than half the patients required at least a 10 month life prolongation to be “worth it.” But about 15% of patients said that even a one month life prolongation would be “worth it.”
So what needs to be done is to take the time to have a conversation with patients — telling them the facts, and, if the facts suggest that one alternative to consider is to stop receiving chemotherapy, to then be prepared to spend as much time explaining the alternatives as is necessary, and this includes considerations such as living wills and possible hospice care. Again, there will never be a net financial (or emotional) incentive to the doctor to withhold potentially beneficial treatment in any case, and counseling about living wills and advance directives is often appropriate, even when the decision is made to continue treatment.
As I have repeatedly stated, it’s legitimate to argue over language and details, but it’s a travesty to claim that this would involve death panels, and it was inaccurate of you to claim that end of life counseling would be “mandatory” and to claim that the legislation contained a coercive “use it or lose it” provision.
– Larry Weisenthal/Huntington Beach, CA
@mata (#166,167,168) My reply went to spam. Again, I won’t have the opportunity to check formatting or revise if it doesn’t display or read properly. I want to make sure that the block quotes and “strongs” are in the right place — maybe someone can look it over and correct the formatting, if I got it wrong. – Larry W/HB
Does anyone really realize from where the word “Behemoth ” comes from? Behemah in Hebrew is a beast (untamed and wild) or a form of monster! Behemoth is actually the translation of “many beast” from Hebrew! That is exactly what we are looking at here! Thank you Curt! Good write up! Good comments as well!
another good POST REVIVE FROM THE 2009
how did the OBAMACARE EVOLVE NOW JULY 2013?
that is after all the phoney scandals
J V HOFFMAN
I COME FROM THE FUTURE IN 2014 FEBRUARY, TO TELL YOU HOW TRUE YOU WHERE,YOU DEFINE THE TODAY GROWING BEAST AS WE SPEAK, SHE BEHEMOTH LIVES IN AMERICA, NOW,
BYE
openid.AOL.COM/RUNNSWIM
ON 157 NOVEMBER 18 2009
IS IN IT UNFAIR TO PICK ON THOSE AT THE NEAR END OF LIVES,
TO BE USE IN A CALCULATION OF EARTHLY MONEY COST,
DON’T THOSE WHO HAVE THE TASK COULD NOT PICK ON OTHER FACTS INSTEAD OF THROWING THE BURDEN ON THE ONE WITH A SHORTER TIME TO LIVE,
is in’t theire whole contribution to society not counted as a wealthy gift they have donated
which deserve the best care to prolong their lives no matter the cost they have paid for all their lives
TO GET, NOT OTHERWISE WHICH CALCULATING THE COST OF DAYS LEFT,
EVEN TRYING TO SPEED THE ENDING,SO TO SAVE MONEY,WHICH IS THE BEST TIME TO BE SPEND TO A DESERVING HUMAN JUST BECAUSE HE TRAVEL WITH US IN THIS JOURNEY WHICH HE WAS WORTHY TO BE HUMAN.
YOU COULD SAVE ON VICIOUS MURDERER WHO HAVE KILLED GOOD PEOPLE, BY HANGING THEM
INSTEAD OF KEEPING THEM IN PRISON MANY YEARS HALF ALIVE HAVING THE MIND INVADED BY THE BEAST,AND SO DANGEROUS, HEAVEN FORBID THEY ESCAPE ONE DAY,
YOU WOULD HAVE A RIGHT TO THINK OF SAVING MONEY THAN,
AS I SEE IT’S FOR THE DEMOCRAT MINDED TO TRY TO SAVE ON THE WEAK OF THIS PEOPLE WHO LOST THEIR RIGHT TO SPEAK FOR THEMSELF AND DEPEND ON THE HEALTH SYSTEM FOR
THEIR NEED AT THE END OF THEIR LIVES,
NO REPUBLICANS WOULD EVEN GET SUCH
IDEA IN THEIR MIND, EVEN TODAY 2014